Unit 3: Advanced Topics & Disease Prevention¶
Chapter 3.15: Supplements for Longevity¶
[CHONK: 1-minute summary]
What you'll learn in this chapter:
- Why supplements are a coaching challenge. Why being an "island of sanity" matters
- The evidence hierarchy for supplement claims: Strong, Moderate, Preliminary, and Speculative
- What the Core Stack (Vitamin D, Magnesium, Omega-3s, Creatine) actually shows in research
- How to discuss advanced molecules (NMN/NR, Berberine) without prescribing
- Third-party testing: what certifications mean and why quality matters
- Scope-safe language patterns for supplement conversations
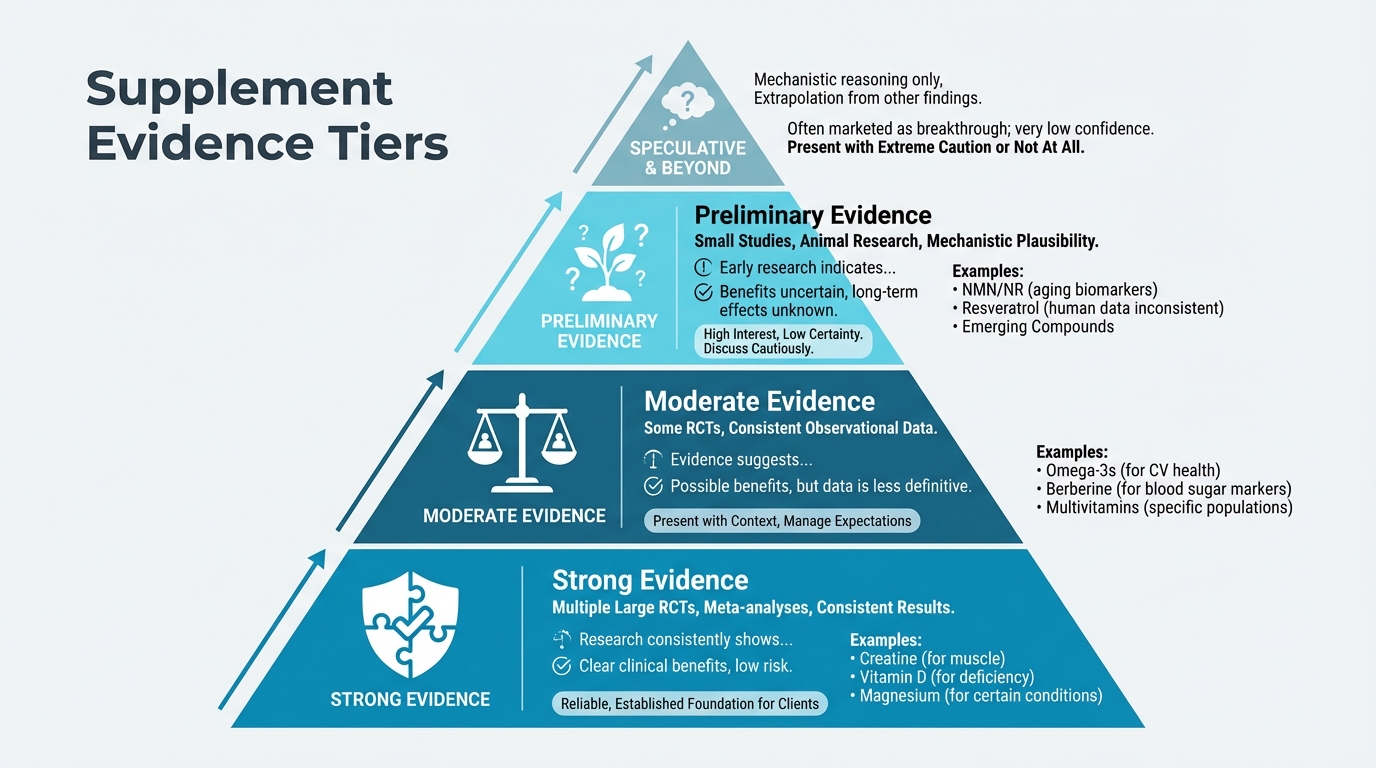
Figure: Strong/Moderate/Preliminary evidence categories
The big idea: In a world drowning in supplement marketing, your clients need a guide who can help them separate signal from noise. This chapter won't tell you which supplements to recommend. That's outside your scope. Instead, it equips you to educate clients about what the evidence actually shows, help them evaluate claims critically, and know when to refer to healthcare providers. The fundamentals—sleep, nutrition, exercise, connection—deliver far more than any supplement stack. Your job is to help clients understand that supplements are, at best, marginal additions to a solid foundation, not shortcuts that compensate for missing basics.
[CHONK: The Supplement Reality Check]
The supplement reality¶
Walk into any health food store, scroll any wellness influencer's page, or listen to popular health podcasts, and you'll encounter an overwhelming message: supplements are essential for health and longevity. The marketing is compelling, the testimonials are passionate, and the promises are dramatic.
And most of it outpaces the evidence by a considerable margin.
This creates a genuine challenge for coaches. Your clients are interested in supplements. Many already take them, and approximately 75 percent of U.S. adults use dietary supplements regularly. They'll ask your opinion. They'll want to know what you think about the latest molecule they heard about on a podcast. They'll wonder if they're "missing out" on something important.
Your job isn't to be dismissive or cynical about supplements. Some have real evidence behind them. Your job is to be an island of sanity, someone who can help clients navigate the gap between marketing claims and actual research.
The marketing-evidence gap¶
In the supplement industry, marketing routinely runs years ahead of evidence.
Under the Dietary Supplement Health and Education Act (DSHEA), supplements are regulated as foods, not drugs. They don't require FDA approval for safety or efficacy before hitting store shelves. Manufacturers can make "structure/function" claims ("supports immune health") without randomized controlled trials to back them up.
This creates an environment where excitement spreads faster than data.
Consider this pattern: A promising mechanism is identified in cell cultures or animal models. Early, small human studies show interesting biomarker changes. Marketing departments run with it. By the time large, well-designed trials publish their results—often showing much smaller effects than expected, or no effect at all—millions of people are already taking the supplement.
Research shows that in four out of five cases, negative clinical trial results have little or no effect on supplement sales. Once people believe something works, evidence to the contrary rarely changes behavior.
This isn't because people are foolish. It's because hope is powerful, marketing is sophisticated, and critically evaluating scientific claims takes skills most people were never taught.
If learning about all this feels a bit unsettling, that's completely understandable. Most coaches (and clients) are surprised when they see how far marketing can drift from the science.
The fundamentals-first hierarchy¶
Before we discuss any supplement, let's establish one key idea: fundamentals deliver far more than supplements.
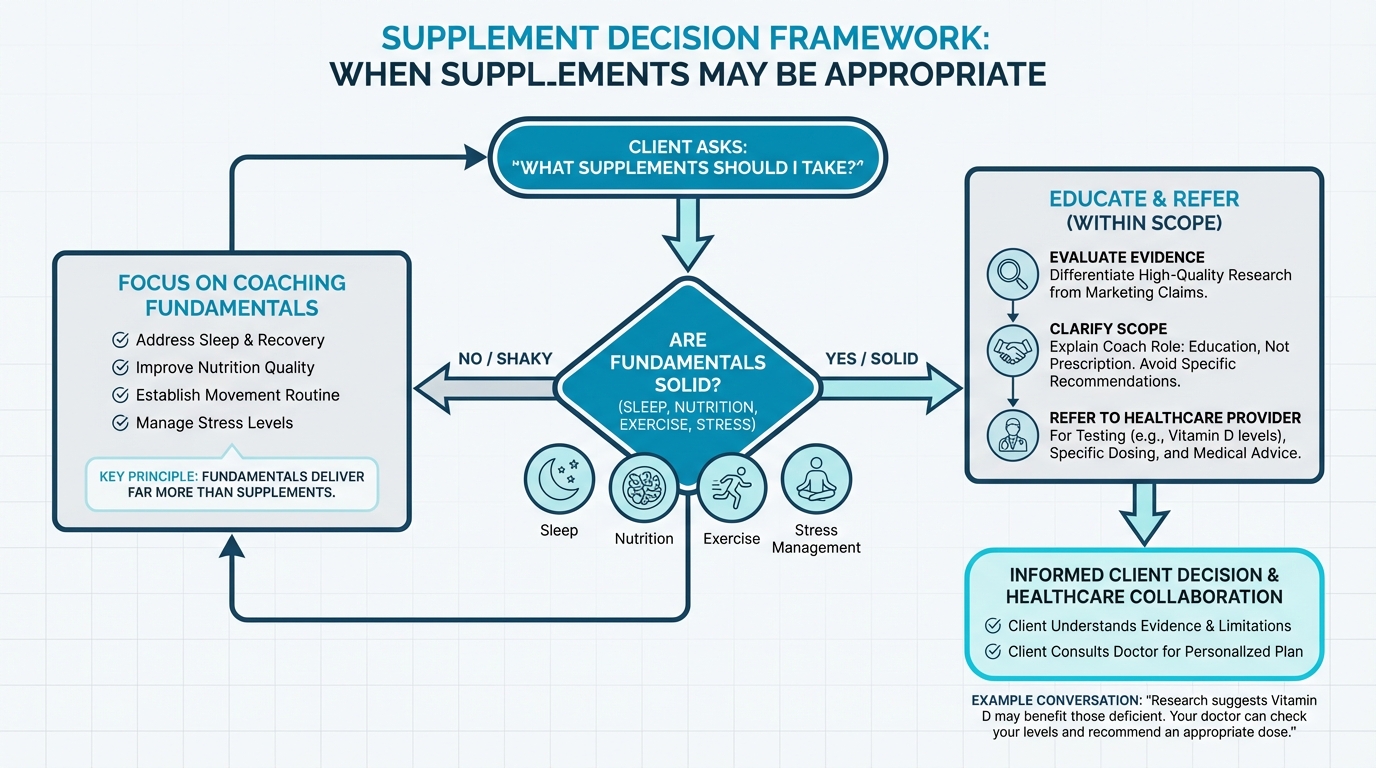
Figure: When supplements may be appropriate
Large epidemiological studies consistently show that combined healthy diet, physical activity, adequate sleep, and weight management can extend disease-free life expectancy by approximately 8 to 10 years. That's a massive effect size.
Compare that to the best-supported supplement findings:
- Vitamin D supplementation shows a modest all-cause mortality reduction of about 5 percent in meta-analyses
- Omega-3 supplementation shows a cardiovascular mortality reduction of about 7 percent
These are meaningful, but they're marginal gains on top of a solid foundation. They're not substitutes for fundamentals.
If a client is obsessing over their supplement stack but sleeping five hours a night, eating mostly ultra-processed foods, and never exercising, supplements aren't the answer. Getting them to address fundamentals would deliver dramatically more benefit than any supplement protocol ever could.
Key phrase to remember: "This is nice-to-have, not need-to-have."
What this means for your client¶
When clients ask about supplements, your first instinct should be curiosity about their fundamentals:
- How's their sleep? (Seven to nine hours, consistent timing?)
- How's their nutrition? (Adequate protein, vegetables, minimally processed?)
- Are they exercising? (Strength training, cardiovascular work?)
- How's their stress? (Chronic overwhelm impacts everything)
- Are they connected? (Social isolation is a major health risk)
If any of these fundamentals are significantly off, that's where coaching attention belongs first. Supplements are "extra credit," meaningful only after the basics are solid.
[CHONK: The Core Stack: Evidence-Based Supplements]
Understanding evidence levels¶
Before examining specific supplements, we need a way to think about different types of evidence when evaluating claims. Not all evidence is equal, and responsible education requires labeling what we know versus what we're guessing.
| Evidence Level | What It Means | How to Present |
|---|---|---|
| Strong | Multiple large RCTs, meta-analyses, consistent results | "Research consistently shows..." |
| Moderate | Some RCTs, consistent observational data | "Evidence suggests..." |
| Preliminary | Small studies, animal research, mechanistic plausibility | "Early research indicates... but more study is needed" |
| Speculative | Mechanistic reasoning only, extrapolation from other findings | Present very cautiously or not at all |
Most supplement marketing presents preliminary evidence as if it were strong. Your job is to help clients understand the difference.
If these categories feel a bit abstract right now, that's okay. You'll get more comfortable with them as we keep coming back to them throughout the chapter.
| For DIY Learners |
|---|
| Applying this to yourself: Before taking any supplement, ask yourself: What's my evidence hierarchy? Have I solidified sleep (7+ hours)? Exercise (150+ min/week with strength training)? Nutrition basics (adequate protein, vegetables, limited UPFs)? Stress management? If not, focus there first. The "fundamentals-first" principle applies to you, too. A $200/month supplement stack on top of 5 hours of sleep and no exercise is a poor investment. |
Vitamin D¶
Evidence Level: Moderate (for mortality); Strong (for deficiency correction)
Vitamin D supplementation is perhaps the most studied supplement for health outcomes, with a substantial body of randomized controlled trial data.
What research shows¶
A 2023 meta-analysis of 80 randomized trials with approximately 163,000 participants found that vitamin D supplementation reduced all-cause mortality by about 5 percent (odds ratio 0.95). That's a statistically significant but modest effect.
Importantly, vitamin D showed no significant effect on cardiovascular mortality or major cardiovascular events in this and other large meta-analyses. So the mortality benefit appears to come from other causes: possibly cancer, respiratory illness, or other pathways.
The effect is likely strongest in people who are actually deficient. Blood levels below 20 ng/mL (50 nmol/L) are considered deficient, and deficiency is common, especially in northern latitudes, darker-skinned individuals, older adults, and those who spend limited time outdoors.
Protocol reference¶
Research typically uses doses of 2,000 to 5,000 IU daily for adults. This aligns with what many longevity-focused physicians recommend. However, individual needs vary based on baseline status, sun exposure, body weight, and other factors.
What this means for your client¶
Vitamin D is one of the more evidence-based supplements, particularly for people who are deficient or at risk of deficiency. But it's not a magic bullet. The effect size is modest, and it doesn't replace fundamentals.
The coaching conversation might sound like: "Vitamin D has some of the better evidence among supplements, especially if you're low. Many people benefit from having their levels checked by their doctor, who can recommend an appropriate dose based on your specific situation."
Magnesium¶
Evidence Level: Moderate (for specific outcomes); Mixed (for mortality)
Magnesium is involved in over 300 enzymatic reactions in the body, including energy production, muscle function, and nervous system regulation. Deficiency is relatively common. Surveys suggest a substantial portion of the population doesn't meet recommended dietary intake.
What research shows¶
The picture is a bit more complex: The evidence differs dramatically between dietary magnesium and supplemental magnesium.
Dietary magnesium: A dose-response meta-analysis found that higher dietary magnesium intake is associated with lower all-cause mortality, about 6 percent lower risk for every additional 100 mg per day from food.
Supplemental magnesium: The same analysis found no significant association between supplemental magnesium and all-cause mortality.
Why the difference? Possibly because dietary magnesium comes packaged with other nutrients and fiber from whole foods. People who eat magnesium-rich foods (leafy greens, nuts, seeds, whole grains) tend to have overall healthier diets. The magnesium itself might not be the active ingredient. It might be a marker of diet quality.
However, magnesium supplementation does show benefits for specific outcomes in randomized trials:
- Blood pressure: Reductions of approximately 3-4 mmHg in trials
- Cardiometabolic markers: Improvements in various risk factors
- Sleep quality: Some evidence of improvement, particularly with magnesium glycinate or threonate forms
Forms matter¶
Magnesium comes in many forms with different absorption and effects:
- Magnesium glycinate: Well-absorbed, often used for sleep and relaxation
- Magnesium threonate: Marketed for cognitive function; crosses blood-brain barrier
- Magnesium citrate: Good absorption; can have laxative effect
- Magnesium oxide: Poorly absorbed; primarily laxative effect
If keeping track of all these forms feels confusing, you're not alone. Clients don't need to memorize every type; they just need help asking good questions of their healthcare provider about what might suit their situation.
Protocol reference¶
Research and longevity protocols typically reference doses of 300 to 600 mg daily, depending on form and individual needs.
What this means for your client¶
Magnesium supplementation may help people who are deficient or seeking specific benefits like blood pressure support or sleep improvement. But the mortality benefit seems to come primarily from dietary sources, not pills.
The coaching angle: "Getting magnesium from food—leafy greens, nuts, seeds—seems to be associated with better outcomes than supplements. If someone's interested in supplementing, that's a conversation for their healthcare provider, especially regarding form and dose."
Omega-3 fatty acids (EPA/DHA)¶
Evidence Level: Moderate (for cardiovascular outcomes)
Omega-3 fatty acids, particularly EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid), have been studied extensively for cardiovascular health.
What research shows¶
A large meta-analysis of randomized trials found that omega-3 supplementation:
- Reduced cardiovascular mortality by about 7 percent (relative risk 0.93)
- Reduced risk of nonfatal heart attack and coronary heart disease events
- Showed stronger effects for EPA-only formulations versus combined EPA/DHA (about 18 percent reduction for EPA-only)
However, the picture isn't entirely rosy:
- Omega-3 supplementation increased risk of atrial fibrillation by about 26 percent
- Bleeding risk also increases
This is a genuine benefit-risk tradeoff that varies by individual. Someone with existing cardiovascular risk factors and no history of arrhythmia might benefit. Someone with atrial fibrillation might not.
Dose matters¶
Most of the positive cardiovascular trials used doses of 1 to 4 grams of EPA/DHA daily, which is far more than what most over-the-counter fish oil capsules provide. A standard fish oil capsule might contain only 300-500 mg of combined EPA/DHA.
Protocol reference¶
Longevity-focused protocols typically reference 2 grams of combined EPA/DHA daily. Achieving this often requires multiple capsules or concentrated formulations.
What this means for your client¶
Omega-3s have meaningful cardiovascular evidence, but the benefit-risk calculation is individual. The dose in most supplements is often too low to match what trials used.
For clients interested in omega-3s: "This is definitely one to discuss with a healthcare provider, who can consider your cardiovascular risk, any history of arrhythmias, and whether the dose you're taking actually matches what the research used."
Creatine¶
Evidence Level: Strong (for muscle); Preliminary (for cognition)
Creatine is one of the most studied supplements in sports nutrition, with decades of research on muscle performance and strength.
What research shows¶
For muscle: The evidence is strong. Creatine supplementation improves strength, power, and muscle mass when combined with resistance training. This is well-established across numerous studies and meta-analyses.
For cognition: This is newer and more preliminary. A 2024 meta-analysis found small but significant improvements in short-term and working memory with creatine supplementation. The effects appear larger in:
- Older adults
- Vegetarians/vegans (who get less creatine from diet)
- People under stress or sleep-deprived
Importantly, there's no mortality data for creatine. The cognitive benefits are intriguing but based on smaller, shorter studies.
Protocol reference¶
Standard dosing is 3 to 5 grams daily for maintenance (some protocols reference up to 10 grams). A "loading phase" of higher doses isn't necessary. It just reaches saturation faster.
What this means for your client¶
For clients doing resistance training, creatine has solid evidence for muscle-related benefits. The cognitive angle is interesting but still developing.
Unlike some supplements where evidence is thin, creatine actually has strong research behind it for its primary use case. The emerging cognitive research is intriguing, particularly for older adults, but needs more confirmation.
B-Vitamins¶
Evidence Level: Context-dependent (Moderate for deficiency; Weak for general supplementation)
B-vitamins (B6, B9/folate, B12) are essential for energy metabolism, neurological function, and red blood cell formation. Deficiency can cause significant health problems.
What research shows¶
B-vitamin supplementation is most clearly beneficial when deficiency exists:
- B12 deficiency is common in older adults (reduced absorption), vegans/vegetarians (dietary source is animal products), and those taking certain medications (metformin, proton pump inhibitors)
- Folate deficiency during pregnancy increases risk of neural tube defects
- B6 deficiency can cause neurological symptoms
For the general population without deficiency, evidence for B-vitamin supplementation reducing disease risk or mortality is weak. Large trials have generally found no cardiovascular or cognitive benefit from B-vitamin supplementation in non-deficient populations.
Protocol reference¶
Protocol content references B-vitamins (especially B6, B9, B12) as part of the core stack, recognizing that suboptimal intake is common.
What this means for your client¶
B-vitamin supplementation makes most sense for people at risk of deficiency: older adults, vegans/vegetarians, those on certain medications, and pregnant women (for folate specifically). For others, a diet including animal products, legumes, and leafy greens typically provides adequate B-vitamins.
CoQ10 (Coenzyme Q10)¶
Evidence Level: Moderate (for specific populations); Weak (for general use)
CoQ10 is a compound involved in cellular energy production, particularly in the mitochondria. It also has antioxidant properties.
What research shows¶
CoQ10 has meaningful evidence in specific contexts:
- Statin users: Statins reduce CoQ10 production, and some studies suggest supplementation may help with statin-related muscle symptoms
- Heart failure: Meta-analyses show CoQ10 may improve symptoms and reduce hospitalizations in people with heart failure
- Older adults: CoQ10 levels naturally decline with age
For healthy adults without these specific concerns, evidence of benefit is limited.
Protocol reference¶
Optional supplements in longevity protocols often include CoQ10 at 100-300 mg daily.
What this means for your client¶
CoQ10 has a reasonable rationale for people taking statins or those with heart failure, though it should be discussed with their healthcare provider. For generally healthy adults, the evidence is much weaker.
Coaching in practice: "What supplements should I take?"¶
The scenario: Your client comes in excited (and a little overwhelmed) after listening to several health podcasts.
Client: "I keep hearing about all these supplements on podcasts. What should I be taking for longevity?"
What NOT to do:
❌ Immediately start listing specific products, doses, or brands.
Why it doesn't work: You'd be stepping outside your scope, and you'd also be skipping over the fundamentals that matter far more for their long-term health.
What TO do:
✅ Validate their interest, then gently redirect to the fundamentals-first hierarchy.
Sample dialogue:
Coach: "That's a great question, and I can share what the research shows. Before we get into specific supplements though, I'm curious about your foundation. When I look at the evidence, the biggest returns come from sleep, nutrition, exercise, and stress management. Supplements are more like extra credit once those are solid. How's your sleep been lately?"
Client: "Honestly? Not great. I’m up late most nights and probably get about five or six hours."
Coach: "Got it—that's really common. The good news is, improving sleep, nutrition, and movement can do far more for your longevity than any supplement stack. If we focus there first, then later on we can talk about how to have a good conversation with your doctor about whether any supplements make sense for you. How does that sound?"
Key takeaway: This approach:
- Validates their interest without dismissing it
- Redirects to the fundamentals-first hierarchy
- Opens a conversation about where coaching can actually help
- Stays within scope (no supplement recommendations)
[CHONK: Advanced Molecules: Education Without Recommendation]
The "biohacking" world¶
Beyond the Core Stack, a whole category of "advanced" supplements has emerged in longevity circles. These are the molecules that generate excitement on podcasts, fuel extensive online discussion, and often carry premium price tags.
The evidence for most of these is preliminary at best. But clients will ask about them, so you need to understand what the research actually shows, and doesn't show.
A critical mindset shift¶
Before we discuss any of these molecules, remember:
No supplement has been proven to extend human lifespan.
Not one. Zero. The excitement around these compounds comes from animal studies, mechanistic reasoning, and short-term biomarker changes in small human trials. None of them have demonstrated that they help humans live longer.
This isn't being pessimistic. It's being accurate. When discussing these with clients, this context matters enormously.
If that feels a bit discouraging, you're not alone. Many clients are surprised to learn how limited the evidence is so far.
NAD+ precursors (NMN and NR)¶
Evidence Level: Preliminary
NAD+ (nicotinamide adenine dinucleotide) is a coenzyme essential for cellular energy production and various metabolic processes. NAD+ levels decline with age, which has generated significant interest in boosting them.
NMN (nicotinamide mononucleotide) and NR (nicotinamide riboside) are precursors that the body can convert to NAD+.
What research shows¶
Human trials consistently demonstrate that both NMN and NR supplementation increase blood NAD+ levels. This is well-established.
What's less clear: whether raising blood NAD+ translates into meaningful health benefits.
A 2022 trial of NMN in 80 adults over 60 days found improved 6-minute walk distance at the highest dose (900 mg/day). That's encouraging but represents a single study.
Multiple reviews conclude that while NMN and NR reliably increase NAD+ in blood, clinical benefits are "limited or inconsistent" across trials. Some show improvements in certain outcomes; others don't.
Expert consensus from a 2025 scientific conference emphasized:
- Current research is limited by lack of tissue-specific NAD+ measurement
- No head-to-head trials comparing NMN versus NR
- More phase 3/4 clinical trials are needed before broad recommendations
If you're feeling a bit lost in the details of NAD+ metabolism, that's okay. You don't need to master every mechanism to help clients keep their expectations grounded.
Safety¶
Both compounds appear safe in short-term studies at tested doses (100-1,250 mg/day for NMN; similar ranges for NR). No serious adverse events have been reported in published trials.
What podcasts say versus what research shows¶
| What podcasts often claim | What research actually shows |
|---|---|
| "NMN reverses aging" | NAD+ levels increase; no human longevity data exists |
| "Essential for anyone over 40" | Benefits unclear; most healthy adults haven't been studied long-term |
| "Dramatic energy improvements" | Some trials show modest functional improvements; others show nothing |
What this means for your client¶
If clients are already taking NAD+ precursors, there's no strong evidence they're causing harm. But there's also no strong evidence they're providing meaningful benefit for most people.
These are expensive supplements with preliminary evidence. For clients considering them: "The research is interesting but still early. No one has shown these extend human lifespan. If you're curious, it's worth discussing with your healthcare provider, and making sure your fundamentals are solid first, since those have much stronger evidence."
A note on antioxidant supplements¶
Evidence Level: Weak to Harmful
Given the marketing focus on "fighting free radicals" and "oxidative stress," we need to address antioxidant supplements directly.
What research shows¶
This is where marketing and evidence diverge dramatically. The Cochrane Collaboration's systematic review of antioxidant supplements for mortality prevention found:
- No protective effect from antioxidant supplements (beta-carotene, vitamins A, C, E, selenium) on overall mortality
- In the most rigorous trials (low bias risk), beta-carotene increased mortality by about 5 percent
- Vitamin E also increased mortality by about 3 percent in low-bias trials
This finding has been consistent across multiple large reviews. High-dose antioxidant supplementation may actually cause harm.
It's understandable if that feels counterintuitive given how often antioxidants are marketed as "anti-aging." Many clients are surprised to learn that more isn't always better here.
Why might antioxidants cause harm?¶
Paradoxically, some oxidative stress appears beneficial. The body uses reactive oxygen species for signaling and adaptation. Exercise, for example, creates oxidative stress that triggers beneficial adaptations. Taking high-dose antioxidants might blunt these adaptive responses.
What this means for your client¶
Clients taking antioxidant supplements "for health" may be surprised to learn the evidence suggests they're either useless or potentially harmful. Getting antioxidants from food (fruits, vegetables, spices) doesn't carry the same concerns. Food-based antioxidants come in balanced amounts with other beneficial compounds.
This is a clear case where the fundamentals (eating colorful vegetables and fruits) outperform the supplement shortcut.
Berberine¶
Evidence Level: Preliminary to Moderate (for metabolic markers); No longevity data
Berberine is a compound found in several plants and has been used in traditional Chinese medicine for centuries. It's often marketed as "nature's metformin" because of its effects on blood sugar.
What research shows¶
For metabolic health specifically, berberine has more human evidence than most advanced supplements:
- Meta-analyses show significant improvements in fasting blood glucose, HbA1c, and insulin resistance in people with type 2 diabetes
- When combined with metformin, berberine showed additive benefits
- Lipid improvements (lower triglycerides and LDL, higher HDL) are also documented
However:
- Most studies are relatively short-term
- Studies are geographically concentrated (primarily from China)
- No longevity or hard clinical outcome data exists
Safety¶
Generally well-tolerated, with gastrointestinal side effects being most common. However, berberine can interact with multiple medications, including those metabolized by the same liver enzymes.
What this means for your client¶
Berberine has more metabolic evidence than many "biohacking" supplements, but it's still not a substitute for evidence-based medical treatment for diabetes. Anyone with blood sugar concerns should be working with a healthcare provider, not self-treating with supplements.
Other Optional Supplements¶
The supplements below appear in various longevity protocols and have emerging research interest. Evidence levels range from preliminary to moderate for specific outcomes. As with all supplements, these are "extra credit" after fundamentals are solid, and any decisions should involve a healthcare provider.
Curcumin¶
Evidence Level: Preliminary to Moderate (for inflammation)
Curcumin is the active compound in turmeric. It has anti-inflammatory properties and appears in many longevity protocols.
What research shows:
- Meta-analyses show modest reductions in inflammatory markers (CRP, IL-6) in various populations
- Poor bioavailability without enhancement (black pepper/piperine or lipid formulations)
- Most benefits seen in populations with elevated baseline inflammation
Protocol reference: 1g daily with black pepper or an enhanced-absorption formulation.
What this means for your client: Curcumin may have a role for people with elevated inflammation markers, but it's not a substitute for addressing root causes of inflammation (sleep, stress, diet quality, body composition). Discuss with a healthcare provider, especially if taking blood thinners or other medications.
Vitamin K2¶
Evidence Level: Preliminary (for bone/cardiovascular health)
Vitamin K2 (menaquinone) is distinct from K1 and plays a role in calcium metabolism, helping direct calcium to bones rather than arteries.
What research shows:
- Observational studies link higher K2 intake to lower cardiovascular and all-cause mortality
- Limited RCT data for hard outcomes
- May work together with vitamin D for bone health
Protocol reference: 200mcg daily (MK-7 form most studied).
What this means for your client: K2 has theoretical appeal for bone and cardiovascular health, particularly alongside vitamin D. Evidence is preliminary. Anyone on blood thinners should discuss with their physician, as vitamin K affects clotting.
Sulforaphane¶
Evidence Level: Preliminary
Sulforaphane is a compound found in cruciferous vegetables, especially broccoli sprouts. It activates Nrf2, a pathway involved in cellular defense and detoxification.
What research shows:
- Activates cellular stress-response pathways in human studies
- Some evidence for reducing inflammatory markers and improving metabolic parameters
- Highly variable between supplements; whole-food sources (broccoli sprouts) may be more reliable
Protocol reference: 60-120mg daily (or equivalent from broccoli sprout consumption).
What this means for your client: Sulforaphane is one of the more interesting emerging compounds, but eating cruciferous vegetables likely provides similar benefits with additional nutrients. Supplements vary widely in quality and actual sulforaphane content.
Taurine¶
Evidence Level: Preliminary (for longevity); Moderate (for specific functions)
Taurine is an amino acid with emerging interest in longevity research after a 2023 Science paper showed taurine supplementation extended lifespan in mice and improved healthspan markers.
What research shows:
- Taurine levels decline with age in multiple species
- Animal studies show lifespan extension and improved function
- Human studies show benefits for cardiovascular markers and exercise performance
- No human longevity data yet
Protocol reference: 500-3000mg daily.
What this means for your client: Taurine is generating significant research interest, but human longevity data doesn't exist. It appears safe at typical doses and may benefit cardiovascular and exercise performance. The longevity claims are extrapolated from animal models.
Lion's Mane¶
Evidence Level: Preliminary (for cognitive function)
Lion's Mane (Hericium erinaceus) is a medicinal mushroom with interest in cognitive health and neuroprotection.
What research shows:
- Contains compounds (hericenones, erinacines) that stimulate nerve growth factor in cell studies
- Small human trials show modest cognitive improvements in older adults with mild impairment
- Most studies are small, short-term, and in specific populations
Protocol reference: 1-2g daily of fruiting body or extract.
What this means for your client: Lion's Mane has intriguing mechanisms but limited human evidence. May be worth exploring for clients interested in cognitive support, but expectations should be modest. As always, discuss with healthcare provider.
Ashwagandha¶
Evidence Level: Preliminary to Moderate (for stress/cortisol)
Ashwagandha (Withania somnifera) is an adaptogenic herb traditionally used in Ayurvedic medicine for stress and vitality.
What research shows:
- Meta-analyses show reductions in cortisol and self-reported stress/anxiety
- Some evidence for improved sleep quality
- May support testosterone levels in men (modest effect)
- Generally well-tolerated; rare reports of liver issues at high doses
Protocol reference: 300-600mg daily of root extract (KSM-66 or Sensoril forms most studied).
What this means for your client: Ashwagandha has reasonable evidence for stress reduction. May be useful for clients with elevated stress, though addressing root causes of stress remains more important than supplementation.
Sleep Support Supplements¶
Several supplements have preliminary evidence for sleep support:
Glycine (3-5g before bed): May improve subjective sleep quality and next-day alertness; works by lowering core body temperature.
L-Theanine (100-200mg): Promotes relaxation and alpha brain waves without sedation; often combined with magnesium for sleep.
Apigenin (50mg): A flavonoid found in chamomile that acts as a mild sedative; popularized by Andrew Huberman but limited human trial data.
What this means for your client: These are generally well-tolerated options for clients struggling with sleep. However, sleep hygiene fundamentals (consistency, environment, light exposure, caffeine timing) should be addressed first. Any persistent sleep issues warrant medical evaluation.
Zinc¶
Evidence Level: Moderate (for deficiency correction); Weak (for general supplementation)
Zinc is an essential mineral involved in immune function, wound healing, and hundreds of enzymatic reactions.
What research shows:
- Deficiency is relatively common, especially in older adults, vegetarians/vegans, and those with GI conditions
- Supplementation benefits those who are deficient
- Excessive intake can impair copper absorption and immune function
- No longevity-specific data
Protocol reference: 15-30mg daily (if indicated by deficiency risk factors).
What this means for your client: Zinc supplementation makes sense for those at risk of deficiency. For others, a varied diet typically provides adequate zinc. More is not better: excessive zinc causes problems.
Rapamycin¶
Evidence Level: Speculative (for human longevity)
Rapamycin is actually a prescription medication, an immunosuppressant used in organ transplant recipients and certain cancers. It's received attention in longevity circles because of its dramatic effects on lifespan in animal models.
Brief context¶
Rapamycin inhibits a pathway called mTOR (mechanistic target of rapamycin), which is involved in cell growth and aging processes. In various animal models, rapamycin has extended lifespan more consistently than almost any other intervention.
Some physicians in longevity medicine use low-dose rapamycin off-label, typically under careful monitoring.
Critical points¶
- This is a prescription medication with immunosuppressant effects
- Human longevity data doesn't exist
- Side effects include increased infection risk and metabolic effects
- This is absolutely not something coaches should discuss as if it were a supplement option
We mention it here only because clients may ask about it after hearing podcast discussions. The appropriate response: "That's actually a prescription medication, not a supplement. It's something that would need to involve a physician with specific expertise in this area."
Coaching in practice: When clients bring up podcast claims¶
The scenario: A client comes in quoting an attention-grabbing promise from a popular health podcast.
Client: "I heard on [popular health podcast] that NMN can reverse aging by 20 years. Should I be taking it?"
What NOT to do:
❌ Roll your eyes or dismiss it with, "That's just marketing; it's all nonsense."
Why it doesn't work: The client feels judged or shut down, and you miss an opportunity to teach them how to think critically about claims.
What TO do:
✅ Acknowledge their interest, then separate the hype from the actual evidence.
Sample dialogue:
Coach: "I've heard similar claims. Let me share what we know so far from the research. NMN does reliably increase NAD+ levels in your blood—that part is well-established. What's less clear is whether that translates into meaningful health benefits. The studies so far are small and short-term, and no one has shown it extends human lifespan. The claims about 'reversing aging' are extrapolating way beyond what's been demonstrated."
Client: "So it's not really proven to make you younger?"
Coach: "Right now, no one has shown that in humans. If you're interested in exploring it, that's definitely a conversation for your doctor. I'd also ask how your fundamentals are, because sleep, exercise, and nutrition have far more evidence for healthy aging than any supplement. Would you be open to starting there?"
Key takeaway: This approach:
- Doesn't dismiss the client's interest
- Distinguishes what's proven from what's claimed
- Maintains scope (educates without prescribing)
- Redirects to evidence-based fundamentals
[CHONK: Navigating the Supplement Industry]
Quality matters more than most people realize¶
Even when a supplement has evidence behind it, there's another problem: many products on shelves don't contain what they claim.
The quality problem¶
Research on supplement quality is sobering:
- Independent testing finds that 14 to 50 percent of sports and weight-loss supplements contain undeclared or prohibited substances
- FDA inspections found that about 48 percent of domestic supplement facilities received citations for violations in fiscal year 2023
- The most common violation? Failing to establish specifications for identity, purity, and strength, in other words, not even verifying what's in the product
- Heavy metals (lead, cadmium, arsenic, mercury) are commonly detectable across supplement categories
FDA historically inspected only about 10 percent of supplement facilities annually, and that dropped to around 4 percent after the pandemic.
If those statistics feel a bit alarming, that's a normal reaction. The goal isn't to create fear, but to help you and your clients make more informed, safer choices.
Third-party testing: What the certifications mean¶
Because regulation is limited, independent third-party testing programs have emerged to fill the gap (think of them as extra sets of independent eyes on the manufacturing process). These programs audit manufacturers and test products for quality, purity, and accuracy.
USP Verified (United States Pharmacopeia)
- Requires Good Manufacturing Practice (GMP) audits
- Tests products against established USP standards for identity, strength, and purity
- Includes contaminant screening
- Periodic off-the-shelf retesting
NSF Certified (NSF International)
- Formula and toxicology review
- Contaminant screening (heavy metals, microbes, pesticides)
- Annual facility audits
- NSF Certified for Sport: Additional screening for hundreds of banned substances (relevant for athletes)
ConsumerLab Approved
- Independent off-the-shelf testing
- Tests for identity, strength, purity, and disintegration
- Publishes methods and criteria
- Often uses stricter contaminant limits than other programs (up to 40 times stricter for lead, according to their statements)
An important note on certifications¶
These programs aren't identical. Their criteria differ, and a product might pass one certification while failing another. Certification doesn't guarantee a product is effective, only that it contains what it claims and meets certain purity standards.
Also, absence of certification doesn't necessarily mean a product is poor quality. Many reputable manufacturers don't seek certification due to cost or other business reasons.
Red flags in supplement marketing¶
Help clients recognize warning signs:
Language red flags:
- "Clinically proven" (for supplements, this is often based on very limited data)
- "Revolutionary breakthrough"
- "Doctors don't want you to know"
- "No side effects" (everything has potential side effects)
- Testimonials as primary evidence
Business model red flags:
- Multi-level marketing (MLM) distribution
- Proprietary blends that hide actual doses
- Claims to treat, cure, or prevent disease (illegal for supplements)
- Celebrity endorsements as primary selling point
What this means for your client¶
Clients interested in supplements should:
1. Look for third-party certification (USP, NSF, or ConsumerLab)
2. Be skeptical of dramatic marketing claims
3. Check that doses match what research actually used
4. Discuss any supplements with their healthcare provider, especially if taking medications
The conversation might be: "Quality varies a lot in supplements. One way to increase confidence is to look for third-party certifications like USP or NSF. They indicate the product has been independently tested for quality and purity."
The cost consideration¶
Supplements add up financially. A client taking multiple premium supplements might spend $200-500 per month or more. For many people, that money would deliver far more health benefit if spent on:
- Higher-quality whole foods (more vegetables, better protein sources)
- A gym membership or fitness equipment
- Sessions with a registered dietitian for actual nutrition guidance
- A sleep specialist consultation if sleep is an issue
When helping clients think about supplements, encouraging them to consider opportunity cost is valuable. What else could that money do for their health?
[CHONK: Coaching Supplement Conversations]
Scope-safe language patterns¶
As covered in Chapter 1.5, health and wellness coaches do not prescribe or recommend supplements. The NBHWC scope of practice explicitly states that coaches may share evidence-based information from reputable sources but do not provide nutrition consultation, create meal plans, or recommend supplements.
This boundary exists for good reasons: client safety, legal protection, and professional integrity.
But clients will ask. Here's how to handle it.
What you can do¶
Share evidence-based information:
"Research shows that vitamin D supplementation has modest benefits for mortality, especially in people who are deficient. Meta-analyses suggest about a 5 percent reduction in all-cause mortality."
Help clients evaluate claims:
"When you hear claims like that, it's worth asking: what kind of evidence is this based on? Animal studies? Small human trials? Large randomized controlled trials? The evidence level matters."
Support implementation of provider recommendations:
If a client's doctor has recommended a supplement, you can help them remember to take it, problem-solve barriers, and integrate it into their routine.
Encourage disclosure to healthcare providers:
"Whatever supplements you're taking or considering, it's really important to let your doctor know. Some supplements interact with medications."
Redirect to fundamentals:
"Instead of starting with supplements, I'm curious about your foundation. How's your sleep? Are you hitting your protein targets? Getting regular movement?"
What you cannot do¶
Recommend specific supplements:
- ❌ "You should take vitamin D"
- ✅ "Research suggests vitamin D may benefit people who are deficient. Your doctor can check your levels and recommend an appropriate dose."
Suggest specific doses:
- ❌ "Take 2,000 IU of vitamin D daily"
- ✅ "Research typically uses doses of 2,000 to 5,000 IU. Your healthcare provider can recommend what's right for you based on your levels."
Interpret lab work:
- ❌ "Your vitamin D is low, so you need to supplement"
- ✅ "I see you have those lab results. That's something to discuss with your doctor, who can interpret what they mean for you."
Advise on medication interactions:
- ❌ "That supplement should be fine with your blood pressure medication"
- ✅ "Since you're taking medications, definitely run any supplements by your doctor or pharmacist first. Interactions can be tricky."
When to refer¶
Supplement conversations should trigger referral when:
- Client asks for specific dosing recommendations
- Client has symptoms possibly related to supplement use
- Client takes multiple medications (drug-supplement interaction risk)
- Client has a medical condition that supplements might affect
- Client is pregnant or nursing
- Client wants lab interpretation to guide supplementation
The referral might be to a physician, registered dietitian, or pharmacist depending on the question.
Drug-supplement interactions are real¶
Research shows that approximately 75 percent of U.S. adults use supplements, and many don't tell their healthcare providers. This creates risk because supplement-drug interactions can be clinically significant:
- St. John's Wort reduces effectiveness of many medications including birth control, antidepressants, and blood thinners
- Green tea extract reduced bioavailability of the blood pressure medication nadolol by 85 percent in one study
- Ginkgo biloba increases bleeding risk, especially with blood thinners
- Calcium can reduce absorption of certain antibiotics and thyroid medications
- High-dose fish oil may enhance blood-thinning effects of anticoagulants
Among older adults, 23 to 82 percent concurrently use supplements with prescription medications. In cancer patients, 37 percent had supplement combinations with potential liver interaction concerns.
This is why the referral question isn't just about scope. It's about client safety. Any client on medications should discuss supplements with their healthcare provider or pharmacist.
If trying to remember all these potential interactions feels overwhelming, that's okay. Your role is to notice when supplements and medications overlap and encourage clients to loop in a pharmacist or physician.
Coaching in practice: Handling requests for specific recommendations¶
Client: "Just tell me what you would take. What's your supplement routine?"
Coach: "I really appreciate you asking—that tells me you trust my judgment. What works for me, though, might not be right for you. Our situations are different, and recommending specific supplements isn't something I can do as a coach. That's really a conversation for your healthcare provider who knows your full health picture."
Client: "So you can't just tell me what to take?"
Coach: "I get why that would feel easier. If I just told you what I take, though, I'd be doing you a disservice. Supplements can interact with medications, and what you need depends on things like your lab values, health history, and current prescriptions. What I can do is share what the evidence generally shows and help you think through what questions to ask your doctor. Would that be helpful?"
If the client persists:
Coach: "I know it might seem easier if I just gave you a list, but your safety comes first. Your doctor is really the right person for deciding which specific supplements and doses, if any, make sense for you."
The hierarchy conversation¶
One of the most valuable things you can do is help clients see supplements in proper perspective.
When a client is excited about the latest supplement they heard about, try:
"Before we talk supplements, let's take stock of the foundation..."
- Sleep: Are you getting 7-9 hours consistently?
- Nutrition: Adequate protein? Vegetables? Minimally processed most of the time?
- Movement: Regular exercise including strength training?
- Stress: Is chronic stress being addressed?
- Connection: Are you maintaining social relationships?
"Here's what the research shows about effect sizes..."
- Combined healthy lifestyle: ~8-10 additional disease-free years
- Best-supported supplements: ~5-7 percent relative risk reductions
"Supplements are nice-to-have, not need-to-have..."
- They're extra credit once fundamentals are solid
- They're not substitutes for sleep, nutrition, or exercise
- The fundamentals deliver the biggest returns
For many clients, hearing this is a relief—it means they don't have to chase every new supplement to support their health.
Avoiding supplement anxiety¶
Some clients become anxious about all the things they're "supposed" to be taking. They've heard so many recommendations that they feel overwhelmed or like they're failing.
Your job is to provide relief:
- The fundamentals matter most
- Most supplements have modest or unclear benefits
- Not doing "advanced" protocols doesn't mean they're missing out
- Any progress is meaningful; perfection isn't the goal
What podcasts say versus what research shows¶
This table summarizes common claims versus actual evidence for several popular supplements:
| Supplement | What podcasts often claim | What research actually shows | Evidence Level |
|---|---|---|---|
| NMN/NR | "Reverses aging" | Raises NAD+ levels; clinical benefits inconsistent; no longevity data | Preliminary |
| Berberine | "Natural metformin" | Improves blood sugar markers in diabetics; no outcomes data | Preliminary-Moderate |
| Vitamin D | "Prevents everything" | Modest mortality benefit (~5%); no CV benefit; helps if deficient | Moderate |
| Omega-3 | "Essential for everyone" | Modest CV benefit; increases atrial fibrillation risk; dose matters | Moderate |
| Multivitamins | "Insurance policy" | No mortality benefit in large trials; may slightly reduce cancer incidence | Weak |
| Antioxidants | "Fight aging" | No benefit; beta-carotene and vitamin E may increase mortality | Weak-Harmful |
| Creatine | "Just for bodybuilders" | Strong muscle evidence; emerging cognitive benefits in elderly | Strong (muscle) |
Deep Health integration¶
Supplements intersect with multiple Deep Health dimensions:
Physical: The primary domain: nutrient status, deficiency correction, metabolic support. But physical health depends far more on fundamentals than supplements. The ~8-10 additional disease-free years from combined healthy lifestyle behaviors vastly exceeds any supplement benefit.
Environmental: Quality and sourcing matter. Contamination, heavy metals, and supply chain issues are environmental concerns that affect what's actually in supplement products. Where supplements are manufactured, how they're stored, and what quality controls exist all influence what clients actually consume.
Mental: Supplement culture can create anxiety. The fear of "missing out" on something, the complexity of conflicting information, the expense of stacking multiple products. These create mental burden. Some clients develop what might be called "orthosupplementation" (a kind of perfectionism about pills), an unhealthy fixation on taking the "right" supplements that paradoxically increases stress. Coaches can help reduce this anxiety by providing perspective and emphasizing that no supplement is essential for most people.
Existential: What matters more than supplements? Connection. Purpose. Meaning. Relationships. These aren't sold in capsule form, and they matter more for longevity than any supplement stack. When clients ask about longevity supplements, it's worth gently exploring what they're really seeking. Often, the desire for a "longevity stack" reflects deeper concerns about aging, mortality, or control that are better addressed through reflection and connection than through capsules.
Common supplement myths¶
Before we close, let's address some persistent myths that clients may bring to coaching conversations.
Myth: "If some is good, more is better"¶
This is dangerous thinking with supplements. Many nutrients have U-shaped dose-response curves: too little causes problems, but too much also causes problems. High-dose vitamin E increases mortality risk, and excessive vitamin A can cause toxicity. More is not better.
Myth: "Natural means safe"¶
Plenty of natural substances are toxic. Arsenic is natural. Hemlock is natural. "Natural" is a marketing term, not a safety guarantee. Supplements can cause side effects, interact with medications, and have quality issues regardless of their "natural" origin.
Myth: "Supplements can replace a poor diet"¶
No amount of supplements compensates for a diet of ultra-processed foods. Whole foods contain fiber, phytonutrients, and nutrient combinations that supplements can't replicate. Supplements are, at best, a complement to good nutrition, never a replacement.
Myth: "My favorite health influencer takes these, so they must work"¶
Celebrity and influencer endorsements are marketing, not evidence. Often, influencers are paid to promote products. Even when they're sincere, personal anecdotes don't equal scientific evidence. N=1 doesn't generalize.
Myth: "Expensive supplements are better"¶
Price often reflects marketing budgets more than quality. Some excellent products are affordable; some expensive products fail quality testing. Third-party certification is a better indicator than price point.
Coaching in practice: Helping clients evaluate supplement claims¶
When a client comes to you excited about a supplement claim they've heard, you can turn it into a chance to think things through together.
The scenario: A client brings in an article about a supplement that supposedly "cuts disease risk in half" and wants to know whether to start taking it.
What NOT to do:
❌ Immediately say "Go for it" or "That's bogus" without exploring anything about the claim.
Why it doesn't work: You either become a cheerleader or a skeptic, instead of helping the client build their own critical thinking skills.
What TO do:
✅ Walk them through a few simple questions about the evidence behind the claim.
Sample dialogue:
Coach: "It definitely sounds appealing. Rather than jumping in or writing it off, want to look at the claim together for a minute?"
Client: "Okay, sure."
Coach: "First, what kind of evidence is this based on? Is it animal studies, small human trials, or large randomized controlled trials? Cell culture and mouse studies often don't translate to humans."
Coach: "Second, what were the actual outcomes they measured? Did it affect things that really matter—like death, disease, or quality of life—or just surrogate markers like blood levels of some molecule?"
Coach: "Third, how large was the effect? A 50% increase sounds dramatic, but 50% of a tiny number is still tiny. What's the absolute risk reduction, not just the relative one?"
Coach: "Fourth, who funded the research? Industry-funded studies of industry products deserve extra scrutiny. That doesn't mean they're wrong, but bias is possible."
Coach: "And finally, what do authoritative reviews say? Single studies can mislead. It's helpful to see what systematic reviews and meta-analyses conclude."
Client: "I’ve never thought about it that way. That makes the claim seem a lot less clear-cut."
Coach: "Exactly. You don't have to become a scientist, but asking these questions helps you make more informed choices instead of just accepting a headline."
Key takeaway: Guiding clients through these questions teaches them to think critically rather than automatically believing every supplement claim they hear.
[CHONK: Study guide questions]
Study guide questions¶
Here are some questions that can help you think through the material and prepare for the chapter exam. They're optional, but we recommend you try answering at least a few as part of your active learning process.
-
Why is the "fundamentals-first" hierarchy important when discussing supplements with clients?
-
What's the difference between "strong" and "preliminary" evidence, and why does this distinction matter for supplement claims?
-
A client is excited about a new supplement they heard about on a popular health podcast. What questions would you encourage them to ask about the evidence?
-
What do third-party certifications like USP and NSF indicate about a supplement product? What don't they indicate?
-
What are three situations that should trigger a referral to a healthcare provider when discussing supplements?
-
How would you explain to a client why you can't recommend specific supplements or doses?
Self-reflection questions:
-
Look at your own supplement routine (if you have one). Can you articulate the evidence level for each supplement? Are any of them "sand" that you're taking before solidifying your "Big Rocks"?
-
Where do you get your supplement information? How do you evaluate whether a source is trustworthy versus marketing-driven?
Chapter exam¶
Open-book exam. Select the best answer for each question.
1. According to large meta-analyses, vitamin D supplementation shows:
a) Strong reduction in cardiovascular mortality
b) Modest (~5%) reduction in all-cause mortality
c) No effect on any mortality outcome
d) Benefit only in people with normal vitamin D levels
2. What is the key difference between dietary magnesium and supplemental magnesium regarding mortality?
a) Supplemental shows stronger benefit than dietary
b) Dietary is associated with lower mortality; supplemental shows no association
c) Both show equal benefit
d) Neither shows any mortality association
3. Omega-3 supplementation has been shown to:
a) Reduce cardiovascular mortality but increase atrial fibrillation risk
b) Have no cardiovascular effects
c) Eliminate heart disease risk
d) Reduce all-cause mortality by 25%
4. What does the evidence show about NAD+ precursors (NMN/NR) and human longevity?
a) They extend human lifespan by 10-20%
b) They reliably increase NAD+ levels but haven't been shown to extend human lifespan
c) They have no effect on NAD+ levels
d) They only work in people over 60
5. Under DSHEA, dietary supplements:
a) Require FDA pre-market approval for safety and efficacy
b) Are regulated as drugs with strict requirements
c) Are regulated as foods and don't require FDA pre-market approval
d) Must prove they extend lifespan before marketing
6. Which statement best describes what third-party certifications (USP, NSF) indicate?
a) The supplement is guaranteed to be effective
b) The product contains what it claims and meets certain purity standards
c) The FDA has approved the supplement
d) Clinical trials support the product's health claims
7. A client asks, "What supplements should I take?" The scope-appropriate response is:
a) Share your personal supplement routine
b) Recommend specific products and doses
c) Share evidence-based information and encourage discussion with their healthcare provider
d) Dismiss the question since supplements don't work
8. What proportion of sports and weight-loss supplements may contain undeclared or prohibited substances, according to testing research?
a) Less than 1%
b) About 5%
c) 14-50%
d) Over 75%
9. The "fundamentals-first" principle suggests that:
a) Supplements should be the first intervention
b) Sleep, nutrition, exercise, and stress management deliver greater benefits than supplements
c) Only fundamental supplements like multivitamins matter
d) Clients should avoid all supplements until fundamentals are perfect
10. A client taking multiple prescription medications wants to start a new supplement. The appropriate coaching response is:
a) Help them research which supplements are safe with their medications
b) Recommend they discuss with their healthcare provider or pharmacist before starting any supplement
c) Tell them supplements are natural so interactions don't occur
d) Create a supplement plan that avoids their medication times
11. What evidence level would be appropriate for a supplement claim based only on animal studies and mechanistic reasoning?
a) Strong
b) Moderate
c) Preliminary
d) Speculative
12. Creatine has strong evidence for which benefit?
a) Extending human lifespan
b) Improving muscle strength and power with resistance training
c) Curing cognitive decline
d) Replacing exercise
13. The phrase "nice-to-have, not need-to-have" in supplement discussions means:
a) Supplements are luxury items only wealthy clients should consider
b) Supplements are marginal additions to a solid foundation, not essential requirements
c) Supplements are nice but never have any benefits
d) Clients need to take supplements to have nice health outcomes
14. Which of the following is an appropriate way to share supplement information within coaching scope?
a) "You should take 2,000 IU of vitamin D daily"
b) "Research suggests vitamin D may benefit people who are deficient; your doctor can check your levels"
c) "Your vitamin D is low based on this lab work, so start supplementing"
d) "I take vitamin D so you probably should too"
15. Combined healthy lifestyle factors (diet, exercise, sleep, weight management) have been associated with approximately how many additional disease-free years?
a) 1-2 years
b) 4-5 years
c) 8-10 years
d) 15-20 years
Works cited¶
References¶
-
Ruiz-García A, Pallarés-Carratalá V, Turégano-Yedro M, Torres F, Sapena V, Martin-Gorgojo A, et al. Vitamin D Supplementation and Its Impact on Mortality and Cardiovascular Outcomes: Systematic Review and Meta-Analysis of 80 Randomized Clinical Trials. Nutrients. 2023;15(8):1810. doi:10.3390/nu15081810
-
Mirza AM, Almansouri NE, Muslim MF, Basheer T, Uppalapati SV, Lakra S, et al. Effect of vitamin D supplementation on cardiovascular outcomes: an updated meta-analysis of RCTs. Annals of Medicine & Surgery. 2024;86(11):6665-6672. doi:10.1097/ms9.0000000000002458
-
Bagheri A, Naghshi S, Sadeghi O, Larijani B, Esmaillzadeh A. Total, Dietary, and Supplemental Magnesium Intakes and Risk of All-Cause, Cardiovascular, and Cancer Mortality: A Systematic Review and Dose–Response Meta-Analysis of Prospective Cohort Studies. Advances in Nutrition. 2021;12(4):1196-1210. doi:10.1093/advances/nmab001
-
Henriksen C, Aaseth JO. Magnesium: a scoping review for Nordic Nutrition Recommendations 2023. Food & Nutrition Research. 2023;67. doi:10.29219/fnr.v67.10314
-
Khan SU, Lone AN, Khan MS, Virani SS, Blumenthal RS, Nasir K, et al. Effect of omega-3 fatty acids on cardiovascular outcomes: A systematic review and meta-analysis. eClinicalMedicine. 2021;38:100997. doi:10.1016/j.eclinm.2021.100997
-
Yi L, Maier AB, Tao R, Lin Z, Vaidya A, Pendse S, et al. The efficacy and safety of β-nicotinamide mononucleotide (NMN) supplementation in healthy middle-aged adults: a randomized, multicenter, double-blind, placebo-controlled, parallel-group, dose-dependent clinical trial. GeroScience. 2022;45(1):29-43. doi:10.1007/s11357-022-00705-1
-
Damgaard MV, Treebak JT. What is really known about the effects of nicotinamide riboside supplementation in humans. Science Advances. 2023;9(29). doi:10.1126/sciadv.adi4862
-
Guo J, Chen H, Zhang X, Lou W, Zhang P, Qiu Y, et al. The Effect of Berberine on Metabolic Profiles in Type 2 Diabetic Patients: A Systematic Review and Meta‐Analysis of Randomized Controlled Trials. Oxidative Medicine and Cellular Longevity. 2021;2021(1). doi:10.1155/2021/2074610
-
Jagim AR, Harty PS, Erickson JL, Tinsley GM, Garner D, Galpin AJ. Prevalence of adulteration in dietary supplements and recommendations for safe supplement practices in sport. Frontiers in Sports and Active Living. 2023;5. doi:10.3389/fspor.2023.1239121
-
Li W, Wertheimer A. Narrative Review: The FDA’s Perfunctory Approach of Dietary Supplement Regulations Giving Rise to Copious Reports of Adverse Events. INNOVATIONS in pharmacy. 2023;14(1):7. doi:10.24926/iip.v14i1.4989
-
What Should Dietary Supplement Oversight Look Like in the US?. AMA Journal of Ethics. 2022;24(5):E402-409. doi:10.1001/amajethics.2022.402
-
Loftfield E, O’Connell CP, Abnet CC, Graubard BI, Liao LM, Beane Freeman LE, et al. Multivitamin Use and Mortality Risk in 3 Prospective US Cohorts. JAMA Network Open. 2024;7(6):e2418729. doi:10.1001/jamanetworkopen.2024.18729
-
Macpherson H, Pipingas A, Pase MP. Multivitamin-multimineral supplementation and mortality: a meta-analysis of randomized controlled trials. The American Journal of Clinical Nutrition. 2013;97(2):437-444. doi:10.3945/ajcn.112.049304
-
Bjelakovic G, Nikolova D, Gluud LL, Simonetti RG, Gluud C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Sao Paulo Medical Journal. 2015;133(2):164-165. doi:10.1590/1516-3180.20151332t1
-
Hu FB. Diet strategies for promoting healthy aging and longevity: An epidemiological perspective. Journal of Internal Medicine. 2023;295(4):508-531. doi:10.1111/joim.13728
-
O'Connor EA et al.. Vitamin, Mineral, and Multivitamin Supplementation to Prevent Cardiovascular Disease and Cancer: A Systematic Evidence Review for the U.S. Preventive Services Task Force. USPSTF; 2022. https://www.uspreventiveservicestaskforce.org/uspstf/document/final-evidence-summary/vitamin-supplementation-to-prevent-cvd-and-cancer-preventive-medication
-
Xu C, Bi S, Zhang W, Luo L. The effects of creatine supplementation on cognitive function in adults: a systematic review and meta-analysis. Frontiers in Nutrition. 2024;11. doi:10.3389/fnut.2024.1424972
-
Marshall S, Kitzan A, Wright J, Bocicariu L, Nagamatsu LS. Creatine and Cognition in Aging: A Systematic Review of Evidence in Older Adults. Nutrition Reviews. 2025. doi:10.1093/nutrit/nuaf135
-
NBHWC. Health & Wellness Coach Scope of Practice. National Board for Health & Wellness Coaching; 2023. https://nbhwc.org/scope-of-practice/
-
NIH Office of Dietary Supplements. Dietary Supplements: What You Need to Know. 2023. https://ods.od.nih.gov/factsheets/DietarySupplements-Consumer/
-
Srinivasan VS. Challenges and scientific issues in the standardization of botanicals and their preparations. United States Pharmacopeia's dietary supplement verification program—A public health program. Life Sciences. 2006;78(18):2039-2043. doi:10.1016/j.lfs.2005.12.014
-
Supplement and Vitamin Certification. Available from: https://www.nsf.org/consumer-resources/articles/supplement-vitamin-certification
-
About ConsumerLab.com Testing. Available from: https://www.consumerlab.com/about/
-
Why Your Doctor Needs to Know What Supplements You're Taking. Available from: https://health.clevelandclinic.org/should-i-tell-my-doctor-what-vitamins-i-take
-
Frenkel M, Morse MB, Narayanan S. Addressing Patient Requests to Add Dietary Supplements to Their Cancer Care—A Suggested Approach. Nutrients. 2023;15(24):5029. doi:10.3390/nu15245029
-
Tilburt JC, Emanuel EJ, Miller FG. Does the Evidence Make a Difference in Consumer Behavior? Sales of Supplements Before and After Publication of Negative Research Results. Journal of General Internal Medicine. 2008;23(9):1495-1498. doi:10.1007/s11606-008-0704-z
-
Imai S, Pirinen E, Sack MN, Treebak JT, Tzoulis C, Bruzzone S, et al. From Bench to Clinic: The 2024 FASEB Scientific Research Conference on NAD Metabolism and Signaling. Molecular Medicine. 2025;31(1). doi:10.1186/s10020-025-01394-0